Peptide administration routes in animal research represent one of the most consequential methodological decisions a researcher can make. The route chosen doesn't just affect convenience; it shapes bioavailability, onset time, tissue distribution, and the integrity of the data collected. Whether a study is examining body composition changes, immune modulation, or the behavior of growth hormone secretagogues, the delivery method can either validate or quietly undermine the findings. Subcutaneous, intraperitoneal, and oral routes each carry distinct pharmacokinetic profiles, and understanding those differences is foundational to designing reproducible, meaningful preclinical work.
This article is for informational and research purposes only. Nothing here constitutes veterinary advice, medical guidance, or a recommendation to use any compound in any clinical or personal capacity. All content is intended to support the understanding of preclinical research methodology. For research purposes only — not medical advice.
Peptides are structurally fragile molecules. They're chains of amino acids held together by peptide bonds, and those bonds are vulnerable to enzymatic cleavage at almost every stage of transit through a biological system. Proteases in the gut, peptidases in the bloodstream, and first-pass hepatic metabolism can all degrade a compound before it reaches its target receptor. This is not a minor consideration. It's the central challenge that makes route selection so critical in animal research protocols.
Different routes bypass different enzymatic environments. A peptide delivered subcutaneously avoids the gastrointestinal tract entirely and enters systemic circulation through lymphatic and capillary uptake. One delivered intraperitoneally enters a cavity rich in blood vessels and lymphatics, and one delivered orally faces the full gauntlet of digestive enzymes, gastric acid, and hepatic extraction. These aren't interchangeable paths. They produce meaningfully different plasma concentration curves even when the same compound and dose are used.
Researchers working with compounds related to growth hormone regulation, tissue repair peptides, or metabolic modulators need to match the administration route to the research question. A study asking whether a peptide reaches the liver in sufficient concentration has different needs than one asking whether it crosses the blood-brain barrier.
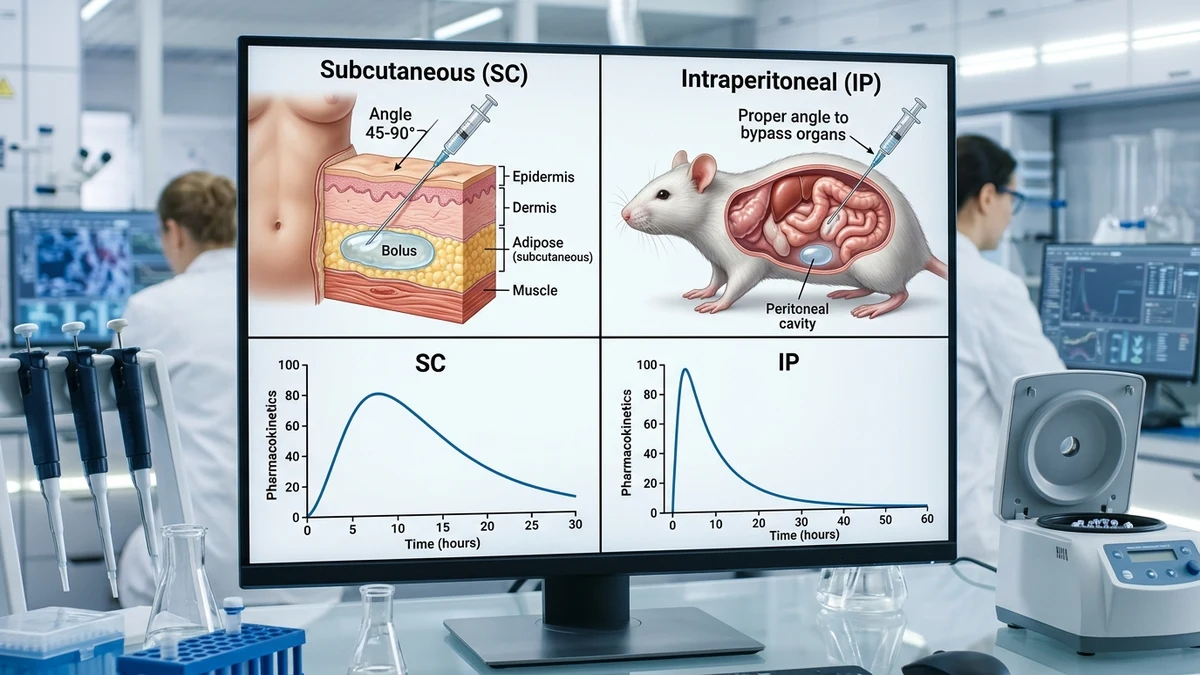
Subcutaneous (SC) injection places a compound into the loose connective tissue beneath the skin, typically at the scruff of the neck in rodent models. It's the most commonly used route for peptide delivery in preclinical research, and for good reason. The absorption is relatively slow and consistent, producing a more extended plasma concentration curve compared to intraperitoneal or intravenous delivery. For many peptides, this slow absorption profile more closely mirrors what a sustained physiological stimulus would look like.
The subcutaneous space has modest vascularity, so uptake depends on diffusion and lymphatic transport. Research suggests that this creates a depot effect for certain formulations, where the compound sits in the tissue matrix and releases gradually. This can be advantageous for studies examining sustained hormonal or anabolic signals, but it introduces its own variable: absorption rate can shift based on injection site perfusion, which changes with ambient temperature and the animal's activity level.
Bioavailability via SC injection varies substantially by peptide. Smaller peptides with stable structures tend to achieve higher bioavailability than larger, more fragile ones. Lipophilicity also plays a role: hydrophilic peptides may not distribute as readily through the interstitial space. According to practitioners working in peptide pharmacokinetics, SC bioavailability for well-characterized research peptides can range widely, and assuming any specific figure without compound-specific data is a common methodological error.
One acknowledged limitation of subcutaneous delivery is site reaction variability. Repeated injections at the same site can produce localized fibrosis, which alters absorption unpredictably. Researchers managing long-duration studies need to rotate injection sites and document this systematically.
Intraperitoneal (IP) injection delivers compound directly into the peritoneal cavity. In rodent research, it's widely used because it's technically simpler than intravenous delivery while still providing rapid and relatively high bioavailability. The peritoneal cavity is lined with a large surface area of vascular tissue, and absorption into the portal circulation occurs quickly. For many water-soluble peptides, IP delivery produces plasma peaks faster than SC routes.
The portal absorption pathway is both an asset and a complication. Compounds absorbed from the peritoneum pass through hepatic first-pass metabolism before reaching systemic circulation, which means peptides susceptible to hepatic degradation will show reduced systemic availability via IP compared to direct intravenous or SC routes. This is an underappreciated nuance. A researcher who switches from IP to SC delivery mid-study without adjusting for this difference may introduce a systematic error that obscures genuine physiological effects.
IP delivery is frequently chosen for studies where rapid onset is desirable, for compounds requiring larger injection volumes than SC tissue can comfortably accommodate, or when researchers are working with solutions that would cause local irritation in subcutaneous tissue. It's also used extensively in immune-related peptide research, where the peritoneal cavity itself contains immune cells and represents a relevant biological environment for the study question.
There are meaningful stress considerations. IP injection in rodents requires restraint and needle penetration into a body cavity, which produces a measurable cortisol response. When studies are examining hormonal axes, metabolic state, or stress-sensitive biomarkers, that cortisol spike is a confounding variable. Short-duration protocols are particularly vulnerable to this problem.
Oral delivery of peptides in animal research presents the steepest bioavailability challenge, and most conventional peptides show minimal intact absorption through the gastrointestinal tract. Gastric acid at low pH begins hydrolysis almost immediately. Luminal proteases, brush-border peptidases, and enterocyte metabolism further degrade the compound before it can be absorbed. By the time residual fragments reach the portal bloodstream, they're often biologically inactive fragments rather than the parent peptide.
So why study it at all? Because oral bioavailability is the holy grail of peptide drug development. A peptide that maintains enough structural integrity to produce a measurable biological effect after oral administration represents a significant research achievement. Studies examining novel formulation strategies, such as nanoparticle encapsulation, cyclization to resist enzymatic cleavage, or peptidomimetic modifications, require oral administration as the test condition. The research question is precisely whether these engineering approaches overcome the bioavailability barrier.
Some naturally occurring bioactive peptides, including certain food-derived sequences and short-chain peptides with specific structural features, do appear to survive GI transit in small fractions. Research suggests this is dependent on molecular weight, charge state, and resistance to specific classes of proteases. The fraction that survives is typically small, but "small" in a biological signaling context isn't always negligible, particularly if the target tissue has high receptor sensitivity.
Oral administration in rodent models also allows researchers to examine gut-level effects directly: receptor binding in the intestinal epithelium, effects on gut peptides like GLP-1 or ghrelin, and local mucosal immune responses. These are legitimate endpoints that SC or IP delivery can't replicate. The route choice, again, must follow the research question rather than convenience alone.
When studies examine peptides with growth hormone secretagogue activity, researchers have noted that SC delivery tends to produce smoother, more physiologically representative GH pulses than IP, which can produce sharper, shorter peaks. For tissue repair and regeneration research, SC is often preferred because local depot formation near target tissue is sometimes intentional. Neurological research, particularly work touching on neuropeptide function, frequently uses IP for its speed of systemic distribution, though some researchers argue for intranasal delivery as an underused alternative for blood-brain barrier access.
Comparative pharmacokinetic studies that have run parallel SC and IP cohorts with the same peptide have consistently found that IP produces earlier Tmax values while SC produces higher or comparable AUC in many cases. The practical implication: if a researcher is trying to model a sustained physiological signal, SC is generally preferable. If the goal is a rapid, defined pulse, IP is more appropriate. These aren't arbitrary preferences; they're conclusions drawn from the pharmacological behavior of the delivery environments.
Oral studies tend to use significantly higher nominal doses to account for absorption losses, which introduces its own interpretive challenge. If a measurable effect occurs after oral delivery, researchers must distinguish between systemic effects from absorbed peptide and local GI effects from unabsorbed compound acting on luminal receptors. Both mechanisms are biologically plausible and scientifically interesting, but they require different experimental controls to separate.
Choosing a route is only the beginning. Injection technique, vehicle selection, and timing relative to feeding state all affect outcomes. Subcutaneous injections in rodents should avoid sites with recently formed fibrous tissue. IP injections require correct needle angle to avoid organ puncture, particularly the cecum, which sits in the lower left quadrant in rats and mice. Oral gavage, the standard method for oral delivery in rodent research, carries aspiration risk and requires trained technique to minimize animal stress and procedural mortality.
Vehicle matters too. Many peptides require specific pH ranges, buffering agents, or carrier molecules to remain stable in solution. Bacteriostatic water, physiological saline, and acetic acid solutions each interact differently with tissue environments, and a vehicle that's appropriate for SC delivery may cause peritoneal irritation at IP injection. Researchers working with novel peptide formulations should conduct preliminary tolerability assessments before committing to a full study design.
Timing relative to feeding is particularly relevant for IP delivery, where a full stomach physically compresses the peritoneal space and may alter compound distribution. For SC delivery, the feeding state matters less mechanically, but metabolic context still shapes how the compound interacts with target tissues once absorbed. These are the small, compounding methodological details that separate clean data from ambiguous results.
The choice of peptide administration route in animal research is not a default to be inherited from prior protocols without scrutiny. Each study has a specific question, a specific compound with specific stability characteristics, and specific endpoints that respond differently to different pharmacokinetic profiles. The researchers who produce the most reproducible and translatable preclinical data are usually the ones who treat route selection as an active methodological decision rather than an afterthought.